

The Healthcare AI Revolution Has Started
Viewing ChatGPT Health vs. Claude for Healthcare through the academic lens of the Vowels of Clinical Design (AEIOU)

For years, LLMs in healthcare lived in a safe zone: pilots, decks, and demos that never had to survive a real user on a real Tuesday.
January 2026 broke that pattern.
OpenAI shipped a dual strategy in the same week: ChatGPT Health for consumers, plus OpenAI for Healthcare for hospitals.1 Days later, Anthropic answered with Claude for Healthcare and an expanded Claude for Life Sciences stack. 2
Now the system has to react. Clinicians, payers, patients, and builders are no longer debating “should LLMs be in healthcare?” They’re dealing with an early version of what it feels like when they are.3
This is the moment Clinical Design starts to matter.
Because models don’t scale in healthcare. Systems do.
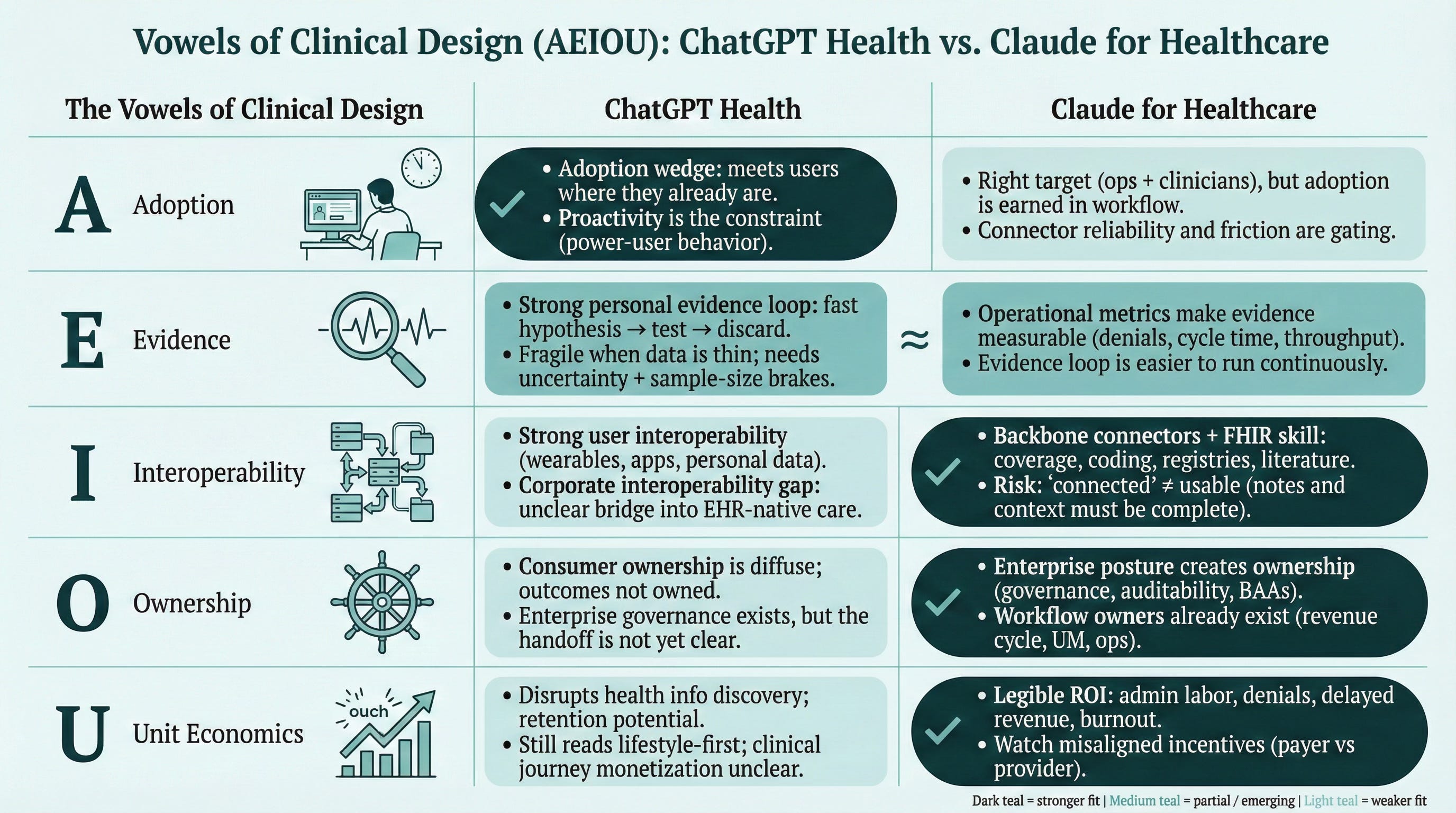
So I’m going to grade these launches using the Vowels framework: AEIOU.
The Vowels of Clinical Design (AEIOU)
A — Adoption: does it show up naturally inside the human moment?
E — Evidence: can it prove value continuously, in messy reality?
I — Interoperability: does data flow with meaning into decision points?
O — Ownership: who holds the pager, the risk, the rollout?
U — Unit Economics: who pays, who benefits, what keeps it alive?
Read my previous article here where I introduce the academic framework of Clinical Design, which will serve as lens throughout this roadmap.
Abstract (TL, DR)
ChatGPT Health is an Adoption wedge. It rides an existing behavior and makes it coherent. Its main constraint is interoperability with the clinical system: it connects well to you, less well to care delivery.
Claude for Healthcare is a systems wedge. It targets the administrative and clinical backbone, with a compliance posture and integration ambition that matches enterprise reality. Its main constraint is friction: if the connector layer feels brittle, it won’t survive frontline usage.
Both are early. The next 3–6 months won’t be decided by model quality. They’ll be decided by who ships the missing vowels.
0) Mapping the strengths of both solutions reveals two very different strategies

I mapped both launches onto a typical patient journey—from lifestyle and prevention, through first symptoms, workup, diagnosis, treatment decisions, operational logistics, follow-up, and long-term recovery. The infographic isn’t trying to predict winners. It’s showing where each product naturally “lives” today, where it’s merely supportive, and where it’s missing the bridge into the clinical moment. The teal intensity is deliberate: darker boxes mark the steps where the product is structurally advantaged; lighter boxes mark where it’s present but not yet workflow-native. Read it as a delivery map—because in healthcare, the model is rarely the constraint. The journey is.
1) ChatGPT Health — AEIOU
We have now analyzed ChatGPT Health with the Vowels of Clinical Design framework developed by Marcos Gallego.
OpenAI’s consumer bet is straightforward: a dedicated Health space in ChatGPT, grounded in personal context via connectors (medical records and wellness apps).4
A — Adoption
This product wins because it formalizes something people already do.
Power users had already been managing health through ChatGPT: uploading labs, histories, preferences, then iterating over time. The launch experience feels like that pattern, with live connectors and a clearer health-native home.5 Chat GPT already fields a massive scale of health usage at consumer level.6
Adoption risk shows up in two places:
1) Seam friction.
Early user reports describe small but real setup quirks (files, web/mobile inconsistencies). In consumer health, the smallest seam becomes the exit ramp. People don’t troubleshoot their wellbeing.
2) Proactivity.
Right now the product shines when the user behaves like a project manager. Example: you ask, “Do my steps correlate with sleep?” then iterate: “What about resting heart rate before bed?” then discard weak hypotheses in seconds.7 That’s powerful for a self-tracker. It’s not how most people behave. If the system can’t surface “what changed” on its own, it will skew toward power users and plateau.
E — Evidence
ChatGPT Health’s best feature is the evidence loop: fast hypothesis testing on your own data.
It’s also where reality bites.
One physician tester reported the model calling a cycle correlation “significant” on n=3, then losing the correlation when pressed to go deeper.8 That’s not a scandal. It’s a design requirement: sample-size awareness, data-quality checks, uncertainty signaling, and a bias toward “insufficient data” when the inputs are thin.
Healthcare evidence doesn’t tolerate confident guesses. Especially when the user doesn’t know they’re guessing too.
I — Interoperability
This is where precision matters: interoperability with what.
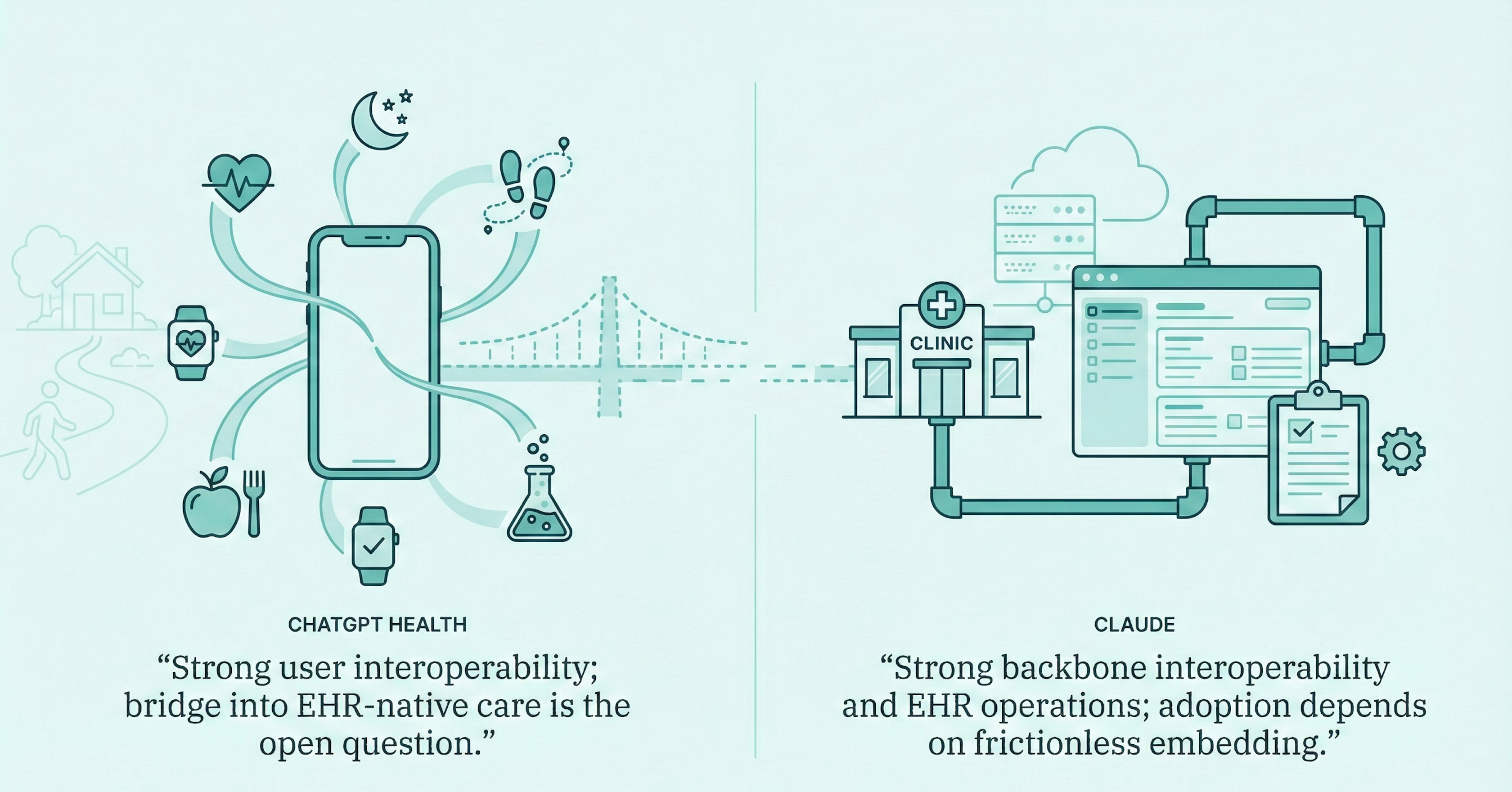
ChatGPT Health is strong on user interoperability: it connects to consumer sources (Apple Health, nutrition apps, wellness platforms) and gives the user a unified conversational layer.
Its weakness is corporate interoperability: the care delivery world. EHR-native workflows. Clinical note text. Provenance. The difference between “I have my labs” and “my care team can act on this.” 9
OpenAI has a separate enterprise answer—OpenAI for Healthcare—so the real question is the bridge: how (and whether) insights can move from the consumer Health space into clinical workflows safely, with consent, audit trails, and accountability. That coexistence is implied, but not yet fully legible in product form.
A clean way to say it: the product currently connects the user to their data better than it connects the user to the system that treats them.
O — Ownership
Consumer ownership is diffuse by default. The user owns the habit. Nobody owns the outcome.
Enterprise ownership exists on paper: governance, compliance, roles, clinical leadership.
The missing piece again is the handoff. Once patient-side intelligence starts influencing clinician behavior, someone needs to own how that intelligence is generated, presented, and trusted.
U — Unit Economics
ChatGPT Health threatens “health information discovery” as a category. Reuters noted that huge volumes of health questions already flow through ChatGPT weekly.
But monetization depends on what it becomes:
a sticky wellness layer that drives retention and paid plans, or
an on-ramp into clinical journeys (referrals, follow-ups, documentation, longitudinal care)
Right now it reads closer to the first. The intention to move into care delivery is visible in the enterprise suite, but the consumer product still looks like it could remain in lifestyle territory.
Net: ChatGPT Health is the Adoption play, with a clinical interoperability gap that will define whether it becomes infrastructure.
2) Claude for Healthcare — AEIOU
We have now analyzed ChatGPT Health with the Vowels of Clinical Design framework developed by Marcos Gallego.
Anthropic’s bet is enterprise-first: HIPAA-ready posture, connectors into the backbone (CMS coverage rules, ICD-10, NPI registry, PubMed), and explicit FHIR development skills.
A — Adoption
The target is right: clinicians and operators want less administrative debt.
Prior auth, claims support, care coordination, coding. These are adoption-positive domains because they’re painful, measurable, and budgeted.
The risk is friction.
A sophisticated clinician reported issues connecting health records through Anthropic’s connector flow—spinners, missing data, unclear manifests, and the model failing to query supposedly ingested records. This is the kind of failure mode that kills usage even when leadership is excited.
Frontline adoption is not won in procurement. It’s won in reliability.
E — Evidence
Claude’s advantage: many of its core use cases have built-in metrics.
Time-to-authorization. Denial rates. Documentation time. Claims throughput. Message triage latency.
Evidence can be continuous because operations already produce the numbers. That’s a strong setup for an evidence loop.
I — Interoperability
This is where Claude is most aligned with Clinical Design.
Connecting to coverage databases, coding systems, registries, and literature isn’t glamour. It’s how products become part of the machine.
The trap is usability: “connected” isn’t enough. Josh Mandel’s note about missing clinical note text is a perfect example of partial reality. Structured FHIR without narrative notes is not what clinicians experience as “the chart.” 10
O — Ownership
Enterprise posture creates ownership: BAAs, access controls, governance, auditability.
Operational workflows also come with owners—revenue cycle, utilization management, clinical ops. That’s why enterprise-first products have a structural advantage in ownership.
U — Unit Economics
Claude has legible ROI because it targets expensive friction:
admin labor
denials and delayed revenue
burnout and turnover
The only landmine is misaligned incentives between payer and provider. Claude will have to sell into the budget owner who captures the value, or prove value is shared.
Net: Claude for Healthcare is the systems play. It will live or die on frictionless embedding and “usable interoperability.”
3) The Comparison: Two Wedges, Two Constraints
OpenAI is trying to turn the patient into the interface, then connect that interface to hospitals.
Anthropic is trying to make the hospital the platform, then extend outward to patients.
So the constraints differ:
ChatGPT Health fights data reality: fragmented records, inconsistent labs, uneven access to EHR-grade context.
Claude for Healthcare fights workflow reality: if ingestion and connectors are brittle, frontline usage collapses.
You can see the mirror:
ChatGPT Health: Adoption ahead of corporate interoperability
Claude for Healthcare: interoperability ambition ahead of frictionless adoption
The Big question: 3–6 Months from Now
Neither of these is designed for the tool graveyard. Not yet.
But in a few months, the shape will be obvious.
Does ChatGPT Health become an on-ramp into care, or stay a self-contained lifestyle layer?
Does Claude turn enterprise readiness into daily reliability, or remain impressive but fragile at the edges?
The healthcare AI revolution won’t be decided by who has the smartest model.
It will be decided by who can ship delivery as a system. By who can ship the vowels.
Why I’m doing this: I believe the next 10 years won’t be defined by who discovers the next molecule, but by who figures out how to deliver it.
Whatever your role (clinician, founder, investor, or policy maker) we are all architects of this new system.
Let’s build.
— Marcos
Note & disclaimers:
Context: The Clinical Decade (and this article) explore the theoretical foundations of Clinical Design, a teaching framework created by Marcos Gallego. It has been developed through independent research and academic activities, and is shared here as a personal contribution to the field.
Independence: Views and materials published in The Clinical Decade are personal/independent and do not represent any employer, client, or institution.
License: Licensed under Creative Commons Attribution–NonCommercial–NoDerivatives 4.0 International (CC BY-NC-ND 4.0), unless otherwise stated.
Reuters — OpenAI launches ChatGPT Health (Jan 7, 2026)
https://www.reuters.com/business/healthcare-pharmaceuticals/openai-launches-chatgpt-health-connect-medical-records-wellness-apps-2026-01-07/
Business Insider — Anthropic launches Claude for Healthcare (Jan 2026)
https://www.businessinsider.com/anthropic-chases-openai-ai-heath-claude-2026-1
Vox — broader analysis of AI + health (Jan 2026)
https://www.vox.com/future-perfect/475081/chatgpt-health-claude-openai-diagnosis-wellness-wearables/
OpenAI PDF — “AI as a Healthcare Ally” (Jan 2026)
https://cdn.openai.com/pdf/2cb29276-68cd-4ec6-a5f4-c01c5e7a36e9/OpenAI-AI-as-a-Healthcare-Ally-Jan-2026.pdf



TechCrunch — OpenAI unveils ChatGPT Health (Jan 7, 2026)
https://techcrunch.com/2026/01/07/openai-unveils-chatgpt-health-says-230-million-users-ask-about-health-each-week/
Simon Smith — “test hypotheses and discard them” (X)


Hillary Lin, MD — “the problem with n=3” (X)

Hillary Lin, MD — post: “This was inevitable…” (LinkedIn)
https://www.linkedin.com/posts/hillarylinmd_this-was-inevitable-openai-has-established-activity-7414788719901323264-wVcL
Josh Mandel, MD — longer write-up: “Health Skillz…” (LinkedIn)
https://www.linkedin.com/pulse/health-skillz-why-i-built-my-own-record-connector-codex-mandel-md-mlz3c
As someone actively trying to optimize personal LLM usage to improve my clinical abilities, this analysis highlights what I've been experiencing: the tools are powerful, but the interoperability gap is real. I'm curious to see whether HIPAA-compliant enterprise deployment actually closes that gap or just creates a different set of frictions. Can Claude for Healthcare do more than help with prior auths? Will it genuinely augment clinical decision-making in the moment, or will the connector issues prevent it from becoming part of the actual workflow?